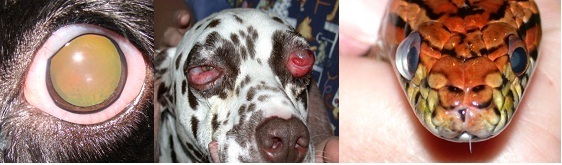
Many see a prominent eye, and think it must be an enlarged (buphthalmic) globe and jump to a diagnosis of glaucoma. This is one possible cause, but there are other possible aetiologies for a prominent eye.
Clinical Signs
The globe looks prominent. In severe cases this is quite obvious, but in early cases this can be hard to define. Try looking from on top, even slight proptosis can usually be identified.
Chemosis: swelling of the conjunctiva is seen when orbital disease leads to reduced venous return. The swollen conjunctiva can dry out, and can also reduce eyelid movement resulting in corneal exposure. A prominent eye with chemosis of the eyelid and or third eyelid conjunctiva suggests retrobulbar disease.
Corneal Exposure: when the globe is quite prominent, the cornea can develop exposure problems. This may be seen as slow healing ulceration, vascular keratitis, and/or pigmentary keratitis.
Reduced Retropulsion: with orbital disease eg tumour, or abscess, or cellulitis, the eyeball cannot be pushed back into the orbit. Compare the affected eye with the normal eye.
How to approach
History: sudden onset, could be glaucoma but for the globe to become enlarged the IOP needs to be increased for some time. Acute onset of a prominent eye suggests either trauma, retrobulbar abscess or cellulitis. Slow progressive exophthalmia in an older animal without pain suggests an orbital tumour.
Check the PLRs: In most cases of orbital disease the PLR is still intact and is usually normal. A normal PLR suggests that the IOP is not increased!
Measure the IOP: The IOP with orbital disease is usually normal at 10 to 25 mmHg. With a glaucomatous, buphthalmic eye the IOP is increased.
Further Diagnostic tests
Further Diagnostic tests for a prominent eye
Ultrasound: can be used to differentiate between solid masses eg a tumour and fluid filled structures such as a retrobulbar abscess or a zygomatic sialocele. The US may also be used to a guide a trucut biopsy or a fine needle aspirate.
X ray: bony changes are suggestive of a tumour. Nasal or sinus adenocarcinomas growing into the orbit or an orbital tumour growing out through the orbital walls into the nasal cavity can be visualized on plain radiographs.
CT scans and NMRI scans: These are the best way to image the orbit, the eye and retrobulbar structures. They usually yield valuable diagnostic information.
Differential Diagnosis
Glaucoma: think breed, red eye, blue eye, with dilated AND non-responsive pupil. For the globe to become enlarged the glaucoma is likely to be chronic. You will then usually also see signs of corneal exposure eg vascular or pigmentary changes. For an enlarged, blind, and potentially painful eye either an ISP—intraocular silicone prosthesis or enucleation is recommended.
Retrobulbar abscess: sudden onset with pain on opening the mouth. Usually young dogs. May need a temporary tarsorrhaphy to protect the cornea from exposure. Most dogs respond well to systemic antibiotics and NSAIDs. Rare that you need to drain these, most discharge spontaneously. Older cats may have underlying dental disease or a necrotic tumour. Young dogs with recurrent retrobulbar abscesses start looking for a foreign body.
Retrobulbar tumour: slow, progressive onset,in an older dog or cat. Use X ray to define any bone involvement. NMRI or CT Scans are very useful to determine the extent of involvement. Orbital surgery may be indicated., usually requires eye removal.
Mucocele, Sialocele: rare. Present with non-painful fluid like swelling usually of the ventral conjunctiva. Aspiration yields salivary secretions. Surgical removal of the zygomatic salivary gland is indicated.
Globe prolapse: eg in a Peke that has been scruffed tightly, or has had trauma. Prompt globe replacement is indicated. Close eyelids with tarsorrhaphy sutures. Leave these in for 10 to 14 days, systemic antibiotics and prednisolone.
Dilated pupil: eg after atropine administration, or a efferent pathway lesion. A widely dilated can give the impression of a prominent globe. Normal retropulsion, normal IOP, view from above the head, and the eye is not exophthalmic.
Chemosis: this may follow allergic reactions, or Chlamydial conjunctivitis in a cat. The swollen hyperaemic conjunctiva may give the impression of a prominent globe.





